- Visibility 190 Views
- Downloads 34 Downloads
- DOI 10.18231/j.jooo.2022.014
-
CrossMark

The relationship between arch, loop and whorl fingerprint patterns with dental caries: A cross-sectional, descriptive institution-based study
- Author Details:
-
 Pooja C Monpara *
Pooja C Monpara *
-
Sima P Odedra
-
Khushali H Shah
-
Vaishali S Dodia
-
Jayasankar P Pillai
-
Sanjay Yadav
Introduction
Dermatoglyphics is the science and specialty of surface markings of the skin particularly feet and hands. The term “fingerprint” refers to an impression of the epidermal ridges of the distal portion of a finger formed on any surface. Fingerprints are distinctive to all individuals and stay unaltered over the lifetime.[1] In old India, edge configuration study was known as ′′Samudra Shastra". The epidermal edge designs were assembled into "Chakra, Shankya and Padma" which relates with the Whorl, Loop and Arch patterns. In India the most punctual review of fingerprint patterns was completed by William Herschel in 1880.[2] The type of fingerprints is unique and is based on the genetic marker of and individuals.[3]
Dermatoglyphic evaluation is a crucial tool for determining the cause of illnesses with a suspected genetic basis early on.[4] In recent years, great progress has been made in linking several types of fingerprint patterns, such as whorl, loop, and arches patterns, with various illnesses, and it has been reported in medicine as a technique of diagnosis.[5] Dermatoglyphic patterns of intrinsic heart diseases, leukaemia, malignant tumours, celiac or gastrointestinal illnesses, schizophrenia, and many sorts of psychological disorders have all been reported. It's also thought to be a sensitive sign of intrauterine problems.[6] This makes fingerprint as an excellent tool for illustrating and screening medical cases.
Dental caries is considered as the most widely prevalent disease in humans. It is a complex illness with multiple etiological causes. It is associated with in the demineralization of the calcified parts and the destruction of the tooth's organic substance by bacterial activity. Saliva (its content and flow), the immunological response of the body, and a reduction in bacterial clearance are all considered as risk factors in caries.[7] It was observed that the caries pattern is comparable in numerous generations of family members; hence, inheritance is postulated.[8], [9] However, environmental factors such as nutrition and dental hygiene habits have a significant role in the development of caries.[10] The dental caries susceptibility due to genetic factors such as structural anomaly in the tooth enamel, tooth morphology, eruption may be reflected by the dermatoglyphics.[11] The present study was designed to evaluate the association between caries prevalence and fingerprint patterns.
Materials and Methods
A total number of 200 patients between the age range of 15 to 40 years were selected from OPD of Government Dental College and Hospital, Ahmedabad. Out of which 150 individuals with dental caries comprised the study group (group 1) and 50 individuals who were caries free comprised the control group (group 2). The caries group were graded for DMFT index according to the WHO standards. Study group were categories by low (group A), medium (group B) and high (group C) caries groups according to DMFT score. Ethical clearance was obtained for the study from the Institutional Ethic Committee (No. IEC GDCH/OP.3/2021). Written permission was obtained through informed written consent forms from the subjects before the clinical examination and recording of fingerprints.
The basic diagnostic instruments along with duplicating ink pads and magnifying glass were used. The recording of finger print was done using the ink pad method in priscribed proforma. The hands of the subject were properly washed with soap and water before being scrubbed with an antibacterial lotion and allowed to dry. The patients' finger tips were pressed into the ink pad 2–3 times before pushing it firmly against the bond paper. While recording the prints, additional care was taken to ensure that the stamp ink material was applied in sufficient amounts. The patient was told to wash his hands with soap and water once the prints were satisfactory. The finger prints were then examined and recorded in a priscribed format.
Patients with skin disorders, devolopmenatal anomalies or injuries in fingertips were excluded from the study.
The finger print patterns and calculated DMFT score for each subjects were entered into a Microsoft Excel Spreadsheet (Version 2109) and statistical analysis was done (Statistical Package for the social Sciences 26.0. IBM Corp).
Results
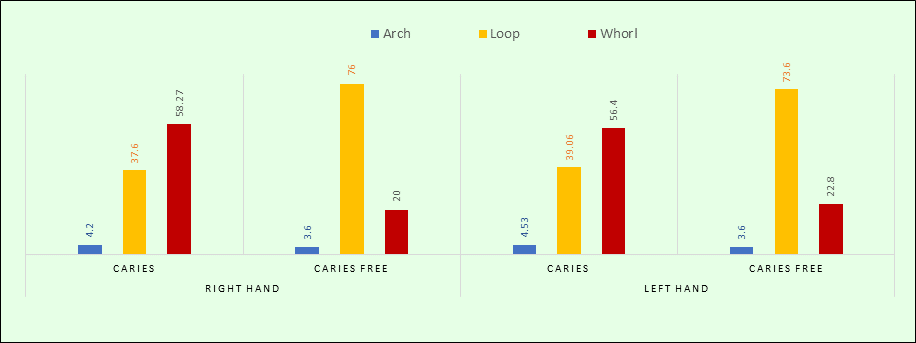
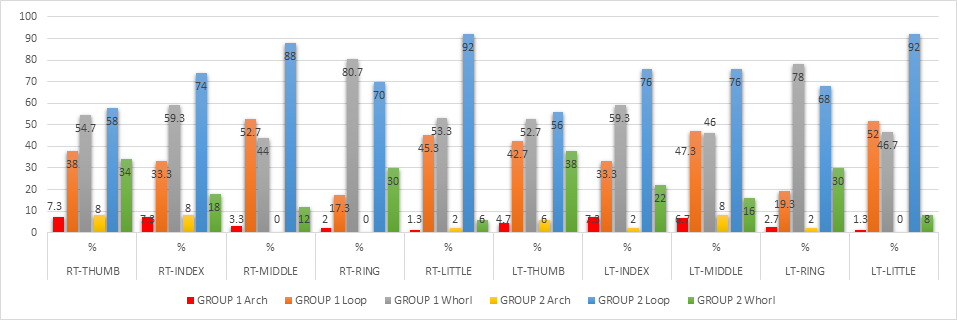
The total of 200 cases were selected for this study. The mean age of subjects was 28.97 years ±6.49 which included 100 males (mean age 28.85 years ±5.98) and 100 females (mean age 29.10 years ± 6.99). The DMFT score of the group 1 ranged from 3 to 12 with the mean score of 4.42±2.90. It was found that group 1 had 57.47% whorl pattern followed by 38.13% loop and 4.4% arch patterns. In group 2, 75% had loop patterns followed by 21.4% whorl and 3.6% arch patterns. Overall sample showed almost equal distribution of whorl and loop patterns and that was 48.45% and 47.35% respectively. The arch pattern was found in only 4.2% of subjects. In group 1, Arch pattern was found maximum (7.3%) in right thumb, right index and left index finger; Loop pattern was maximum (52.7%) in right middle finger; whorl pattern was found maximum (80.7%) in right ring finger. In group 1, compared to all patterns; whorl pattern was found highest in all individual fingers except right middle, left middle and left little, which had increased frequency of loop patterns i.e. 52.7%, 47.3% and 52% respectively. From all fingers right and left ring finger showed maximum whorl patterns and that was 80.7% and 78% respectively. In group 2, all individual fingers showed increased frequency of loop pattern and among them highest loop was found in little fingers (92%) on both sides. Both right and left ring fingers of caries group showed highest difference (63.4%, 58.7%) in relation to loop and whorl pattern compared to other fingers, so it might help maximum in prediction of dental caries.
In both the groups, all the fingers showed statistically significant association between patterns of right and left hands (p<0.001) except middle finger of group 2, among them ring finger of group 1 showed maximum symmetry of both sides in relation to whorl pattern ([Table 1]).
|
Group |
Fingers |
Arch |
Loop |
Whorl |
χ2 |
Sig. |
r |
|||
|
n |
% |
n |
% |
n |
% |
|||||
|
Group 1 Caries Group [N=150] |
Thumb |
6 |
4 |
50 |
33.3 |
68 |
45.3 |
139.69 |
0.000 |
0.632 |
|
Index finger |
5 |
3.3 |
37 |
24.7 |
78 |
52 |
94.677 |
0.000 |
0.647 |
|
|
Middle finger |
3 |
2 |
55 |
36.7 |
52 |
34.7 |
72.182 |
0.000 |
0.611 |
|
|
Ring finger |
1 |
0.7 |
17 |
11.3 |
111 |
74 |
76.467 |
0.000 |
0.691 |
|
|
Little finger |
1 |
0.7 |
59 |
39.3 |
61 |
40.7 |
97.854 |
0.000 |
0.621 |
|
|
Group 2 Caries Free Group [N=50] |
Thumb |
3 |
6 |
24 |
48 |
14 |
28 |
56.969 |
0.000 |
0.745 |
|
Index finger |
1 |
2 |
33 |
66 |
7 |
14 |
31.485 |
0.000 |
0.626 |
|
|
Middle finger |
0 |
0 |
33 |
66 |
1 |
2 |
0.596 |
0.742 |
0.066 |
|
|
Ring finger |
0 |
0 |
30 |
60 |
11 |
22 |
19.225 |
0.000 |
0.604 |
|
|
Little finger |
0 |
0 |
44 |
88 |
2 |
4 |
14.950 |
0.001 |
0.484 |
It was found that loop and whorl patterns showed significant difference between caries and caries free group (p<0.05) whereas Arch pattern was insignificantly different in both the groups (p=0.668) ([Table 2]).
|
Patterns |
Side of hands |
Group |
Z |
Sig. |
|
Arch |
Right |
1 |
-0.332 |
0.740 |
|
2 |
||||
|
Left |
1 |
-0.302 |
0.763 |
|
|
2 |
||||
|
Total |
1 |
-0.429 |
0.668 |
|
|
2 |
||||
|
Loop |
Right |
1 |
-8.116 |
0.000 |
|
2 |
||||
|
Left |
1 |
-7.268 |
0.000 |
|
|
2 |
||||
|
Total |
1 |
-8.131 |
0.000 |
|
|
2 |
||||
|
Whorl |
Right |
1 |
-7.768 |
0.000 |
|
2 |
||||
|
Left |
1 |
-6.939 |
0.000 |
|
|
2 |
||||
|
Total |
1 |
-7.796 |
0.000 |
|
|
2 |
The distribution of DMFT scores was compared with the finger print patterns in each finger. It was found that, the Pearson correlation coefficient (r value) ranged from 0.01 to 0.213. All the fingers, except the right little finger showed a positive correlation, however, the significant correlation was observed only in right middle and ring fingers, left middle, little and ring fingers. Further the results revealed that there was no significant association between DMFT score and the distribution of finger print pattern in all the fingers.
Based on the DMFT scores, the caries group was categorised in to in group A (DMFT 3 to 5), group B (DMFT 6 to 8) and group C (DMFT 9 to 12).
The cross tab of group wise DMFT score and number of arch patterns showed that as the number of arch patterns increased the DMFT score decreased (weak negative correlation, r=-0.113, p>0.05). Only 4% individuals had DMFT score more than 8(group C) with no arch patterns, whereas rest all categorised under under group A and group B. It was observed that as arch pattern increased, DMFT score decreased. ([Table 3])
The cross tab of group wise DMFT score and number of loop pattern showed that as the number of loop pattern increased the DMFT score decreased (negative correlation, r=-0.201) and that to significant correlation (p=0.014) and insignificant association between DMFT score groups and number of loop patterns (p>0.05). Thus, as loop pattern increased, DMFT score decreased similar to the arch pattern. ([Table 4])
The cross tab of group wise DMFT score and number of whorl pattern showed that as the number of whorl pattern increased, the DMFT score also increased (weak positive correlation, r=0.186) and that to significant correlation (p=0.023) and an insignificant association was found between DMFT score groups and number of whorl patterns(p>0.05). Thus, as the whorl pattern increased the chances of dental caries also increased in contrast to the arch and loop patterns.([Table 5] )
|
Total number of arch patterns |
DMFT Score |
χ2 |
Sig |
r |
Sig. |
||||||||||||||||
|
Group A |
Group B |
Group C |
|||||||||||||||||||
|
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
12 |
|||||||||||||
|
% |
% |
% |
% |
% |
% |
% |
% |
% |
36.62 |
0.623 |
-0.11 |
0.17 |
|||||||||
|
1 |
1 |
0.7 |
18 |
12 |
31 |
20.7 |
32 |
21.3 |
17 |
11.3 |
17 |
11.3 |
2 |
1.3 |
2 |
1.3 |
2 |
1.3 |
|||
|
2 |
0 |
0 |
5 |
3.3 |
4 |
2.7 |
2 |
1.3 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|||
|
3 |
0 |
0 |
4 |
2.7 |
0 |
0 |
0 |
0 |
1 |
0.7 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|||
|
4 |
0 |
0 |
2 |
1.3 |
0 |
0 |
4 |
2.7 |
1 |
0.7 |
2 |
1.3 |
0 |
0 |
0 |
0 |
0 |
0 |
|||
|
5 |
0 |
0 |
0 |
0 |
2 |
1.3 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|||
|
6 |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
0.7 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|||
|
Total |
67(44.7%) |
77(51.3%) |
6(4%) |
15.58 |
0.112 |
-0.08 |
0.35 |
|
Total number of loop pattern |
DMFT Score |
χ2 |
Sig. |
r |
Sig. |
|||||||||||||
|
Group A |
Group B |
Group C |
||||||||||||||||
|
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
12 |
63.596 |
0.75 |
-0.201 |
0.014 |
||||||
|
% |
% |
% |
% |
% |
% |
% |
% |
% |
||||||||||
|
0 |
0 |
0 |
3 |
2 |
3 |
2 |
5 |
3.3 |
3 |
2 |
3 |
2 |
0 |
0 |
0 |
0 |
0 |
0 |
|
1 |
0 |
0 |
0 |
0 |
4 |
2.7 |
1 |
0.7 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
2 |
1 |
0.7 |
3 |
2 |
2 |
1.3 |
6 |
4 |
5 |
3.3 |
3 |
2 |
1 |
0.7 |
0 |
0 |
1 |
0.7 |
|
3 |
0 |
0 |
4 |
2.7 |
4 |
2.7 |
5 |
3.3 |
1 |
0.7 |
2 |
1.3 |
0 |
0 |
1 |
0.7 |
1 |
0.7 |
|
4 |
0 |
0 |
6 |
4 |
10 |
6.7 |
9 |
6 |
7 |
4.7 |
8 |
5.3 |
0 |
0 |
1 |
0.7 |
0 |
0 |
|
5 |
0 |
0 |
2 |
1.3 |
4 |
2.7 |
4 |
2.7 |
0 |
0 |
2 |
1.3 |
1 |
0.7 |
0 |
0 |
0 |
0 |
|
6 |
0 |
0 |
2 |
1.3 |
5 |
3.3 |
5 |
3.3 |
3 |
2 |
1 |
0.7 |
0 |
0 |
0 |
0 |
0 |
0 |
|
7 |
0 |
0 |
3 |
2 |
4 |
2.7 |
2 |
1.3 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
8 |
0 |
0 |
5 |
3.3 |
1 |
0.7 |
1 |
0.7 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
10 |
0 |
0 |
1 |
0.7 |
0 |
0 |
1 |
0.7 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
Total |
67(44.7%) |
77(51.3%) |
6(4%) |
21.299 |
0.265 |
-0.175 |
0.032 |
|
Total number of whorl patterns |
DMFT score |
χ2 |
Sig. |
r |
Sig. |
|||||||||||||
|
Group A |
Group B |
Group C |
86.833 |
0.282 |
0.186 |
0.023 |
||||||||||||
|
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
12 |
||||||||||
|
|
% |
|
% |
|
% |
|
% |
|
% |
|
% |
|
% |
|
% |
|
% |
|
|
0 |
0 |
0 |
4 |
2.7 |
1 |
0.7 |
2 |
1.3 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
1 |
0 |
0 |
1 |
0.7 |
0 |
0 |
0 |
0 |
1 |
0.7 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
2 |
0 |
0 |
4 |
2.7 |
1 |
0.7 |
3 |
2 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
3 |
0 |
0 |
3 |
2 |
4 |
2.7 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
4 |
0 |
0 |
1 |
0.7 |
7 |
4.7 |
10 |
6.7 |
2 |
1.3 |
3 |
2 |
0 |
0 |
0 |
0 |
0 |
0 |
|
5 |
0 |
0 |
3 |
2 |
3 |
2 |
2 |
1.3 |
0 |
0 |
2 |
1.3 |
1 |
0.7 |
0 |
0 |
1 |
0.7 |
|
6 |
0 |
0 |
4 |
2.7 |
10 |
6.7 |
10 |
6.7 |
8 |
5.3 |
9 |
6 |
0 |
0 |
1 |
0.7 |
0 |
0 |
|
7 |
0 |
0 |
3 |
2 |
3 |
2 |
2 |
1.3 |
1 |
0.7 |
0 |
0 |
0 |
0 |
1 |
0.7 |
1 |
0.7 |
|
8 |
1 |
0.7 |
3 |
2 |
2 |
1.3 |
5 |
3.3 |
4 |
2.7 |
2 |
1.3 |
1 |
0.7 |
0 |
0 |
0 |
0 |
|
9 |
0 |
0 |
0 |
0 |
3 |
2 |
1 |
0.7 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
10 |
0 |
0 |
3 |
2 |
3 |
2 |
4 |
2.7 |
3 |
2 |
3 |
2 |
0 |
0 |
0 |
0 |
0 |
0 |
|
Total |
67(44.7%) |
77(51.3%) |
6(4%) |
25.448 |
0.185 |
0.169 |
0.049 |
Discussion
The type of fingerprints each person has is unique and is determined by their genetic traits.[3] Dermatoglyphics could indicate a genetic susceptibility to dental caries, Hence the present study was an attempt to evaluate the relationship between these two parameters.
The arch, loop, and whorl patterns were compared in caries and caries-free subjects. The whorl pattern (57.47%) was predominant in caries group compared to caries-free group (21.4%) and Loop pattern was predominant in caries-free (75%) compared to caries group (38.13%). The result of the present study was similar to the finding of a study done by Chinmaya et al. where whorl was 42.85% in the caries group and loop was 57.14% in the caries-free group.[12] This finding was also supported by the previous studies done by Kaur et al, Saxena et al, Sharma and Somani, Gupta, Shivani Duggal et al.[13], [14], [15], [16], [17], [18], [19] Other studies done by Madhusudan et al and Devi et al showed that loop patterns were more prominent in the caries group that is contradictory to the present study.[20], [21] These results might differ from our study because of population variation. In the present study, the ring finger showed the highest whorl pattern followed by the index finger in the caries group compared to other fingers which is supported by a study done by Elkwatehy and Sheta.[22] In the present study, arch pattern was found least in both caries (4.4%) and caries-free (3.6%) groups compared to other patterns. Similar findings were observed in Cheeli et al, and Veeresh et al’s studies.[23], [24] The present study showed a significant difference in fingerprint patterns of both the groups, in which whorl pattern had more frequency in caries group and loop had increased frequency in a caries-free group. These findings were in accordance with studies done by Chand et al, Matar, Reddy et al, and Madan et al.[25], [26], [27], [28] In the present study, Arch patterns had an insignificant negative correlation (-0.08) with dental caries and this finding is supported by the results of Chinmaya et al and Thakkar’s et al studies.[12], [29]
Difference in the results of various studies could be due to the method used to record finger print, environmental factors and difference in the genetic of different study population.
The study has been carried out on a very limited number of participants. It should be done with larger samples between individuals with or without dental caries to establish a relationship between dermatoglyphic pattern variations and dental caries.
Conclusion
The present study concludes that dermatoglyphic patterns differed significantly between patients with dental caries and in controls. An individual's susceptibility to dental caries increases with whorl pattern incidence and lowers with loop pattern incidence. As a result, the examination of fingerprint pattern could be beneficial to assess the susceptibility of an individual to dental caries. Furthermore, large sample population-based studies need to be designed to substantiate the results and to explore further relationship between fingerprint patterns and dental caries.
Source of Funding
None.
Conflict of Interest
None.
References
- B Schaumann, M Alter. . Dermatoglyphics in medical disorders 1976. [Google Scholar]
- DP Mukherjee. How Scientists read palms. Sci Today 1980. [Google Scholar]
- PR Abhilash, R Divyashree, SG Patil, M Gupta, T Chandrasekar, R Karthikeyan. Dermatoglyphics in patients with dental caries: A study on 1250 individuals. J Contemp Dent Pract 2012. [Google Scholar]
- SB Holt. The hypothenar radial arch, a genetically determined epidermal ridge configuration. Am J Phys Anthropol 1975. [Google Scholar]
- JJ Mulvihill, DW Smith. The genesis of dermatoglyphics. J Pediatr 1969. [Google Scholar]
- GA Popich, DW Smith. The genesis and significance of digital and palmar hand creases, preliminary report. J Pediatr 1970. [Google Scholar]
- JR Miller, J Giroux. Dermatoglyphics in pediatric practice. J Pediatr 1966. [Google Scholar]
- CH Lin. Fingerprint comparision I: Similarity of finger prints. J Forensic Sci 1982. [Google Scholar]
- CD Liu, JH Lin, JW Ostrburg, JD Nicol. Finger printcomparison II: Similarity of fingerprints. J Forensic Sci 1982. [Google Scholar]
- TM Hassel, EL Harris. Genetic influences in caries and periodontaldiseases. Crit Rev Oral Biol Med 1995. [Google Scholar]
- WA Bretz. Longitudinal analysis of heritability for dental cariestraits. J Dent Res 2005. [Google Scholar]
- B Chinmaya, B Smitha, S Tandon, C Khurana. Dermatoglyphics: An indicator of dental caries in humans. J Indian Assoc Public Health Dent 2016. [Google Scholar]
- KK Singh, K Menka, K Anand, A Goel, A Dontulwar, JP Rajguru. Correlation between dermatoglyphics and dental caries in children: A case-control study. J Family Med Prim Care 2020. [Google Scholar]
- PH Sanghani, HK Soni, MU Joshi. Correlation of dental caries and dermatoglyphics in pediatric cases. Indian J Dent Sci 2016. [Google Scholar]
- SM Asif, Dbg Babu, S Naheeda. Utility of dermatoglyphic pattern in prediction of caries in children of Telangana Region, India. J Contemp Dent Pract 2017. [Google Scholar]
- R Somani, MP Gupta, S Jaidka, DJ Singh, V Puri, D Kumar. Dermatoglyphics as a Noninvasive Tool for Predicting Dental Caries in Cerebral Palsy and Healthy Children: An In Vivo Study. Int J Clin Pediatr Dent 2019. [Google Scholar]
- A Saxena, D Pradhan, N Pruthi. Dermatoglyphics and dental caries: A correlation study among school children of Kanpur City, India. Rama Univ J Dent Sci 2016. [Google Scholar]
- S Duggal, P Mahajan, P Monga. Dermatoglyphics: A Genetic Marker of Dental Caries. Indian J Forensic Odontol 2019. [Google Scholar]
- A Gupta. Evaluation of correlation between dental caries and fingerprints in known subjects. J Adv Med Dent Sci Res 2019. [Google Scholar]
- K Madhusudan, HP Patel, K Umesh, S Chavan, R Patel, R Patel. Relationship between dermatoglyphics, cheiloscopy and dental caries among dental students of Visnagar town. Int J Adv Res 2015. [Google Scholar]
- M Devi, HAS Sayima, RMT Muthu, S Baburathinam. Role of Rugoscopy and Dactyloscopy in Predilection of Dental Caries in Childern. Indian J Public Health Res Dev 2020. [Google Scholar]
- WM Elkwatehy, AR Sheta. Dermatoglyphics as a non-invasive anatomical marker in early childhood caries. Int J Dentistry Oral Sci 2016. [Google Scholar]
- S Cheeli, KS Kumar, D Dangeti, S Pavanireddy. Comparative Reliability of Rugoscopy and Dactyloscopy for the Predilection of Malocclusion and Dental Caries in Children: A Cohort Study. Braz Res Pediatr Dent Integr Clin 2017. [Google Scholar]
- T Veeresh, A Mujahid, P Deepu, R Sivaprakash. Correlation between dermatoglyphics, dental caries and salivary pH: An invivo study. Ethiop J Health Sci 2019. [Google Scholar]
- SC Chand, HR Parmar, JK Patel, AK Bathvar, MK Garasiya, PK Nisarta. Praiseworthiness of dermatoglyphics in determining dental caries vulnerability among Gujarati children: A cross-sectional study. Natl J Community Med 2018. [Google Scholar]
- MA Matar. Relation between Dermatoglyphicsand Early Childhood caries in a group of Egyptian children. Egypt Dent J 2018. [Google Scholar]
- KV Reddy, KN Kumar, V Subramaniyan, H Togaru, S Kannaiah, R Reddy. Dermatoglyphics: A new diagnostic tool in detection of dental caries in children with special health-care needs. Int J Pedodontic Rehabil 2018. [Google Scholar]
- N Madan, A Rathnam, N Bajaj. Palmistry: A tool for dental caries prediction!. Indian J Dent Res 2011. [Google Scholar]
- VP Thakkar, A Rao, P Rastogi, R Shenoy, G Rajesh, MB Pai. Dermatoglyphics and dental caries: A cross sectional study among 12 year old school children in Mangalore, India. Indian J Forensic Med Pathol 2014. [Google Scholar]