Introduction
A number of morphological variations are observed in human dentition. No two teeth are alike. Teeth play an important role in any anthropological study due to their preservability, observability, variability, and heritability. Teeth also present geographic variability.1
Two kinds of traits have been observed as dental anthropologic structures called metric and nonmetric traits. The nonmetric dental traits (NDTs) are commonly encountered that have high taxonomic importance. They are used to determine the biological relationships among different populations.2
Parastyle or paramolar tubercle is an extra cusp observed on the buccal surface of the mesiobuccal cusp (paracone) of the maxillary molars. In rare cases, parastyle can be observed on the distobuccal cusp (metacone) of the maxillary molars. Similar to other defects in the tooth form, parastyle originates during the morphodifferention stage of tooth development. It develops from an accessory enamel knot on the buccal surface of paracone of maxillary molars.3
Parastyle is rare in occurrence with a prevalence rate of 0–0.1% in maxillary first, 0.4–2.8% in second, and 0–4.7% in the third molars.4 Bolk in 1916 described this rare entity. In 1945, Dahlberg introduced this anomaly in the paleontologic nomenclature, by referring it as parastyle occurring on maxillary molars and as protostylid occurring on the mandibular molars.5 Kustaloghi named this as “upper paramolar structures” or “upper paramolar complex”, with a prevalence rate being lower in maxillary first molars (0%–0.1%) than second (0.4%–2.8%) and third molars (0%–4.7%). These anomalies show a bilateral occurrence in deciduous and unilateral in permanent dentition.6
The parastyle gives an insight to dental development and evolution.7 These anomalies can cause various clinical problems. Hence, it is required to diagnose and plan the preventive or restorative management of anomaly.
This case report is presenting 4 different cases collected randomly within a period of 6 months from a pool of about 4000 patients among the North Indian population, from October 2019 to March 2020, in the Department of Oral Medicine and Radiology, HP Govt. Dental College and Hospital Shimla.
Case Report 1
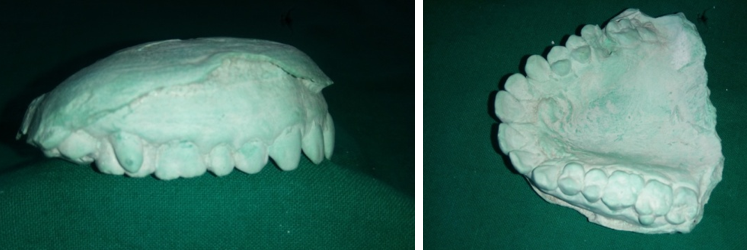
A female aged 34 yrs old reported in the Deparment of Oral Medicine and Radiology with a chief complaint of missing tooth in lower left posterior region and with the desire to fabricate a new fixed prosthesis. The patient’s familial and medical histories were non-contributory. Intraorally there was a tubercle seen on the facial surface of 27 arising from the junction of mesiobuccal and distobuccal cusps covering a major portion of facial developmental groove (Figure 1). The tubercle was cone-shaped, measuring approximately 5.5mm cervicoocclusally and 5 mm mesiodistally, clearly delineated from the associated tooth by a groove. The base of tubercle extends till the gingival margin with apex pointed occlusally, being below the occlusal plane. The cusp tip was found to be round in shape with a deep developmental groove between the tooth surface and free cusp tip. The buccal aspect was smooth, moving downward straight to the cemento-enamel junction (CEJ).
Intraoral periapical (IOPA) radiography of 27 to visualize the parastyle revealed pear shaped radiopacity that is merging with the rest of the tooth in the cervical area (Figure 2, Figure 3 ). There was no root structure evident.
Based on clinical, radiographic findings and with reference to the available literature, a diagnosis of Parastyle occurring on maxillary 2nd molar was made.
As the patient was unaware of the extra cusp and was asymptomatic with no evidence of caries, a periodic follow up every 6 month was advised.



Case Report 2
A female patient, 28-years-old reported to the Department of Oral Medicine and Radiology complaining of food lodgement in lower left posterior region of tooth for the past one month. Family and medical histories were non significant. No abnormalities were detected on extraoral examination. Intraoral examination showed proximal caries in 36, 37 region, with no soft-tissue abnormalities. A parastyle was noticed on the mesiobuccal surface of maxillary right second molar (Figure 4, Figure 6). It was observed to be conical in shape with dimensions 4 mm mesiodistally and 5.5 mm cervicoocclusally, extending below the occlusal plane. IOPA radiograph of 17 showed a V-shaped radio opacity on the mesiobuccal cusp of second molar (Figure 5).


Case Report 3
A 15 yrs old male reported in the Department of Oral Medicine and Radiology with a chief complaint of backwardly displaced upper right front region tooth. The patient’s family and medical history were non-significant. Intraorally there was a tubercle observed on the mesiobuccal cusp of 17 (Figure 7, Figure 8). The tubercle was cone-shaped, with dimension of 4 mm cervicoocclusally and 3 mm mesiodistally, clearly sepereted from the related tooth with a groove. The base of anomaly is present at the gingival margin, with the apex pointing occlusally but below the occlusal plane.
The buccal surface of the tubercle was smooth, moving straight to the cemento-enamel junction (CEJ). A diagnosis of parastyle was therefore made for the tubercle.
Intraoral periapical (IOPA) radiography of 17 to visualize the parastyle revealed cone shaped radiopacity that is merging with the rest of the tooth in the cervical area, with no evidence of root structure.


Case Report 4
A 6 yrs old female reported in the Department of oral Medicine and Radiology with chief complaint of decayed lower back region teeth. Intraorally there is a tubercle seen on the mesiobuccal cusp of left deciduous 1st molar (Figure 9). The tubercle was cone-shaped, with dimensions of 2.5 mm cervico‑occlusally and 2mm mesio distally, clearly separated from the associated tooth by a groove. On the buccal surface, the tubercle forms a triangular prominence with free cusp tip round in shape and oriented occlusally extending half the total length of mesiobuccal cusp and base towards the gingival margin.

Discussion
The extra cups or cusp‑like structures are normal or anomalous structures, with a strong racial predilection and a great importance orally, phylogenetically, and anthropologically. Many theories have been advocated in relation to extra-cusp such as concrescence, differentiation, and tritubercular.8 The etiology for extracusp formation is still unknown. But it has been suggested that these traits are primarily polygenetic with environmental influence.9 PAX and MSX genes are responsible for the abnormal shape of the teeth.10
Recent embryological evidence advocates that morphogenesis of tooth characterized by transient signalling centers in the epithelium, that consist of epithelial cell clusters corresponding to the initiation of individual cusps.11 Parastyle/paramolar cusp/paramolar tubercle is a non-metric dental trait (NDT) referred to as a cingulum present normally on the buccal surface of the paracone of the maxillary molars.12
As these anomalies have a high taxonomic importance, thus they can be used to estimate the differences among populations, related to micro-evolutionary processes, which can give information about ethnic and racial variations.3 Kustaloghi reported a high incidence of parastyle in both the dentitions as compared to the other races, with a low occurrence.6
In 1974, Joseph F Katich and Turner created a scale based on the expression and degree of parastyle, so as to describe the different clinical presentations of this anomaly.13 The scores were:13
Buccal surfaces of the cusps 2 and 3 are smooth (Cusp 2 being paracone/mesiobuccal cusp; Cusp 3 being metacone/distobuccal cusp).
Pit present in or around the buccal groove between cusps 2 and 3.
Small cusp present with attached apex, usually on the cusp 2.
Medium‑sized cusp with free apex present on the buccal surface.
Large cusp with free apex on the buccal surface.
Very large cusp present with free apex on the buccal surface.
Free peg‑shaped crown attached to the third molar root.
The importance of paramolar tubercle is unknown but it may give insights to dental evolution and development. The clinical importance lies in the fact that fissures present between the tooth surface and accessory cusp are prone to dental caries and pulpal involvement, for which they can be restored or treated endodontically.3
Various problems like sensitivity/devitalization due to attrition/fracture, caries, pulpal involvement, periapical disease, difficulty in bracket and crown placement, plaque accumulation etc are encountered with the presence of parastyle or an extracusp.8
During orthodontic management, these paramolar tubercles are often managed by enameloplasty, as they interfere with the bracket placement and cementation.3 Hence, it is important to recognize the anatomical variations associated with teeth.
In our case series, the patients reported with good oral hygiene in spite of the parastyle as they were educated and advised to monitor the area regularly. We have encountered four cases of parastyle, which are of rare occurrence in modern hominids. This will help to increase the awareness among the dental practitioners about this rare anomaly in relation to its diagnosis, management, ethnic variabilities and forensic identification.
Conclusion
The present case series reported with four cases of parastyle present on the maxillary molars, which is rare in occurrence. Reporting of such morphologic anomalies helps in forensic recognition and increases the knowledge of dental practitioners in identification and management of such rare anomalies.