Introduction
The calcifying epithelial odontogenic tumor (CEOT) is rare odontogenic tumour account for less than 1% of all odontogenic tumour and was first introduced into scientific literature almost 50 years ago by Dr. J J Pindborg and thus, is also referred to as the “Pindborg tumor”.1 Histogenesis of the tumor is still not clear, some believe that CEOT arise from the stratum intermedium layer of the enamel organ in the tooth development stage while other pathologist believes that this tumor may arise from remnants of the primitive dental lamina found in the initial stage of odontogenesis from the reduced enamel of embedded tooth or from stratum intermedium of enamel organ.2 We report a case of 24 year female with CEOT in right posterior maxilla.
Case Report
A 24-year female came to the department of Oral Medicine and Radiology with the complain of swelling on right side of middle 3rd of face since 2 years. The swelling was associated with mild pain from the past 3 months. The pain was intermittent and dull aching in nature. Patient went to outside dentist for this, took Ebility and Amoxclav CV (625mg) following which she had mild symptomatic relief. However, after 3 days she experienced mild pain at right posterior maxilla and was refered to our dental school for further evaluation. On general examination, she was well-nourished and moderately built.
On extraoral examination diffuse swelling, was evident in the right middle 3rd of face extending superiorly a line drawn from right ala of nose to tragus of ear and inferiorly right corner of lip to 4 cm below tragus of ear which is mild tender on palpation with normal overlying skin colour and temperature (Figure 1). All the lymph nodes were non palpable.
Intraorally, 15 is palatally placed and 17, 18, 43 are missing. On palpation, there was tenderness in the retromolar area distal to 26 and slight buccal cortical expansion of uniform bony hard consistency in the retromolar region compared to the opposite side (Figure 2).
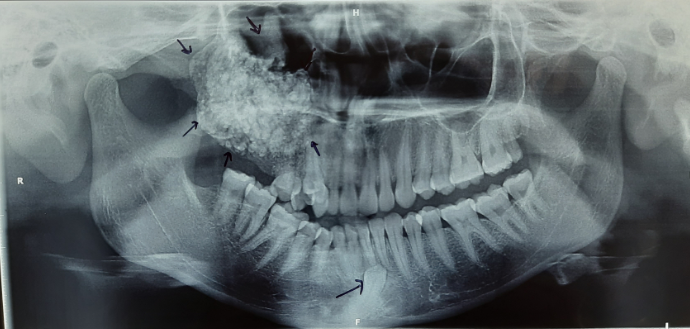
The patient was subjected to radiographic examination. The panoramic view demonstrated a large mixed radiopaque lesion measuring about 6x7 cm in the posterior maxilla extending anteroposteriorly from 15 to distal of maxillary tuberosity and infero- superiorly from right alveolar region to orbital floor (Figure 3).
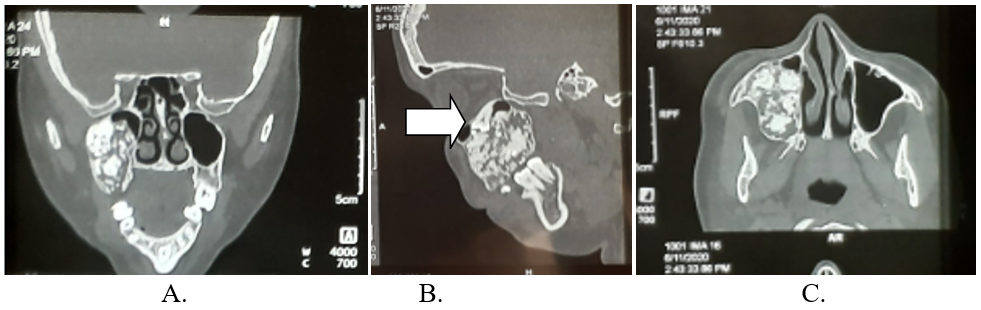
Further assessment with CT scan, there was a large expansile lucent lesion with hyperdense inclusions involving lateral wall of right maxillary sinus likely arising from alveolar region of maxilla along right premolar region. The lesion is displacing the right maxillary sinus medially with an ectopic unerupted tooth superomedially (Figure 4).
Based on the clinical and radiographic findings, a differential diagnosis of Ameloblastic fibrodontome, Calcifying odontogenic cyst (COC) and complex odontome was made.
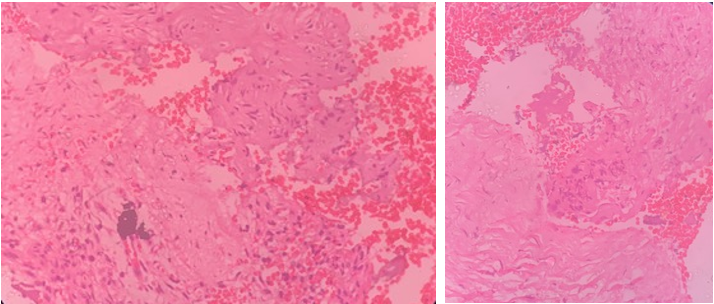
Incisional biopsy was done, from lesion which revealed predominantly hyalinized stroma with extensive areas of dystrophic and cementum like calcification. Few small islands of epithelial cells with areas of hemorrhage are also seen. Histopathological features, are suggestive of Calcifying Epithelial Odontogenic tumour (Figure 3).
Resection of lesion was planned for treatment.


Discussion
CEOT is a rare odontogenic tumour accounts for roughly less than 1% of all odontogenic tumours, has a wide age distribution with a mean of 43.5 years, with equal sex predilection.1 Intraosseous (central) or extraosseous (peripheral) are the variants of CEOT. The frequency of tumor ranges between 4% and 3% in which extra osseous variant constitutes about 6% and intraosseous variant 93.6%. Intraosseous is the most common variant evident in the mandibular premolar/molar region. Intraosseous lesions are larger and more aggressive, which can grow upto 4 cm comparatively to extraosseous lesions which are smaller less than 2 m in diameter and localised involving anterior gingival and diagnosed earlier. In addition to this, peripheral type have low recurrence rate due to their less aggressive nature.3, 4 CEOT usually presents as an asymptomatic benign tumour; however, there may be swelling and non-specific pain depending on lesion size and relationship with neighbouring structures, such as the maxillary sinuses.5 Three – dimesnsional radiographic modalities helps in attaining information about the lesion regarding size of lesion, pattern of growth, calcifications and relation to adjacent structures.
CEOT is often as an incidental radiolographic finding with widely varying radiological features that create diagnostic confusion. Radiographically, its features may appear similar to a dentigerous cyst, adenomatoid odontogenic tumour (AOT), calcifying cystic odontogenic tumour (CCOT), variants of ameloblastoma, odontoma, or a central ossifying fibroma. With current radiographic findings, the dentigerous cyst, AOT and ameloblastoma were excluded as differential diagnoses as these lesions were not consistent with the radiographic presentation of the current case. AOT can appear as a mixed (radiolucent and radiopaque) density lesion, but present in anterior jaws with radiolucencies having scattered radiopaque foci.6, 7, 8 CEOTs that are radiolucent in early stages can also be mistaken for ameloblastomas, but ameloblastoma are mostly found in the posterior mandible, and associated with root resorption and cortical destruction.9, 10 Due to the more radiopacity exhibited in the current lesion, an AOT and ameloblastoma were radiologically excluded from the differential diagnosis.2
Differential diagnosis for this case were made complex odontoma and central ossifying fibroma (COF). Complex odontoma presents as a haphazard radiopaque mass which is surrounded by a radiolucent halo which is also associated with an impacted teeth. COF, on the other hand, often presents as a well-defined mixed density lesion in the mandibular molar regions.10, 11
Radiographically, in CEOT the lesion usually consists of a radiolucent area, which may be well or poorly defined, unilocular or multilocular lesion, containing radiopaque masses of varying size. In current case lesion had high level of tumour maturity and there was considerable expansion with extensive calcification in the lesion gave it a densely radiopaque appearance, which exceeded that usually seen in a CEOT and was more suggestive of a complex odontoma. The lesion in this case displaced the right maxillary sinus medially with an ectopic unerupted tooth. Although CEOT is a benign tumor, it has variable biologic behaviour ranging from mild to moderate invasiveness. The tumour grows by infiltration and produces cortical expansion and root resorption.12
Despite the atypical radiological presentation, the lesion was histopathologically diagnostic of CEOT, displaying the distinctive histological features as described earlier in the histopathological report of the patient. Histopathologically, CEOT is composed of polyhedral neoplastic cells, which have abundant eosinophilic finely granular cytoplasm with nuclear pleomorphism and prominent nucleoli. Most of the cells are arranged in anastomosing sheet-like masses. An extracellular eosinophilic homogenous material staining like amyloid is characteristic of this tumor with concentric calcific deposits called Liesgang ring.13, 14
Treatment of CEOT has ranged from enucleation or curettage to radical and extensive resection such as hemi mandibulectomy or hemimaxillectomy. Treatment plan is dependent on various factors such as size, location. Small lesions are treated by enucleation or curettage. Large tumours require segmental resection, hemimandibulectomy or hemimaxillectomy which causes bone discontinuity reguire reconstruction procedures.2
Conclusion
CEOT is a rare odontogenic tumour that can attain significant growth in the jaws and is often asymptomatic; however, it may also cause symptoms that mimic dental or sinus pain. It maybe confused with radiologically similar lesions such as an odontoma and central ossifying fibroma in mature lesions. Three-dimensional imaging can provide valuable clinical information regarding the nature of the lesion and guide its management. Clinicians should be aware of the range of differential diagnoses for odontogenic jaw lesions, and refer as appropriate for diagnosis and management.